Existing levels of shortages
Pharmacists said that on average they had seen shortages affect 21% of prescription drugs in the last 3 months, with over 90% of respondents feeling that the shortages had increased over the last 12 months.
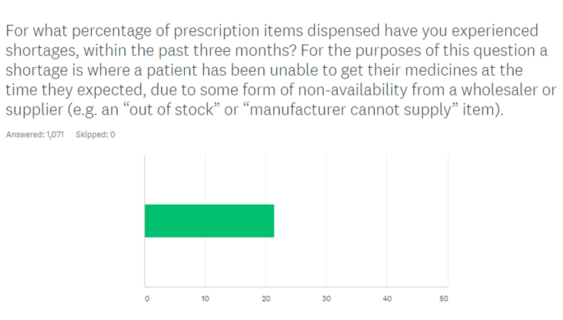
Figure 1: Existing levels of shortages
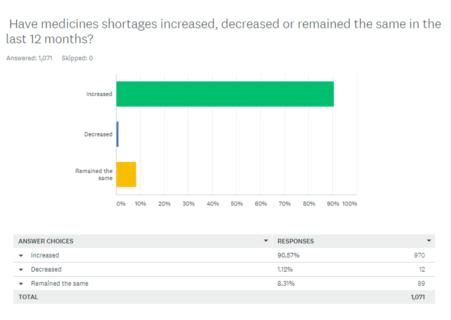
Figure 2: Change over the last 12 months
Time currently spent on dealing with medicines shortages
Dealing with drug shortages is already taking up significant time with 62% of respondents saying they spend an hour or more every day trying to sort out problems caused by medicine shortages.
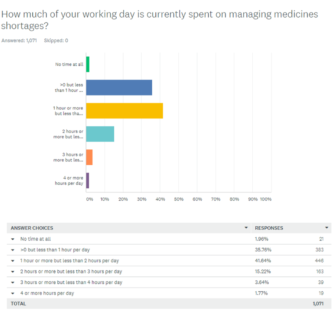
Figure 3: Time currently spent on managing medicines shortages
Consequences of medicines shortages
When we asked about patient harm, 25% said that they were aware of patient harm as a result of shortages.
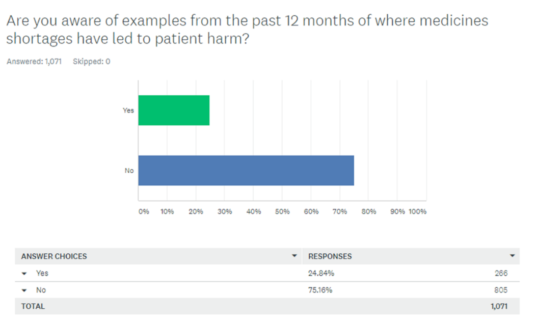
Figure 4: Awareness of patient harm caused by shortages
Examples given of harm to patients included:
- Patients admitted to hospital with anaphylactic shock being unable to take home life-saving adrenaline autoinjectors for future use due to lack of supplies.
- Patients having to carry expired adrenaline autoinjectors as no in date stock was available – with the associated worry that they might not be effective should they be used.
- Patient having to go on holiday with only one adrenaline autoinjector due to delayed delivery from supplier. Patients are advised to always carry two.
- Patients changed to different formulations of their regular blood pressure reducing medicine with loss of blood pressure control.
- One patient changed to a different blood pressure formulation of the same drug suffering a fall leading to bone fractures because their replacement formulation resulted in their blood pressure being lowered too far.
- Patients suffering severe distress and discomfort due to widespread shortages of HRT medication.
- Patients having to go without DOAC* drugs which are used to prevent strokes in at-risk patients.
- Patients suffering seizures due to shortage of anti-epileptic drugs.
*Direct oral anticoagulants.
Consequences of a no-deal Brexit
When asked about the effect of a no-deal Brexit, over 81% of respondents felt that medicines shortages would get worse, with 55% believing they would get ‘much worse’.
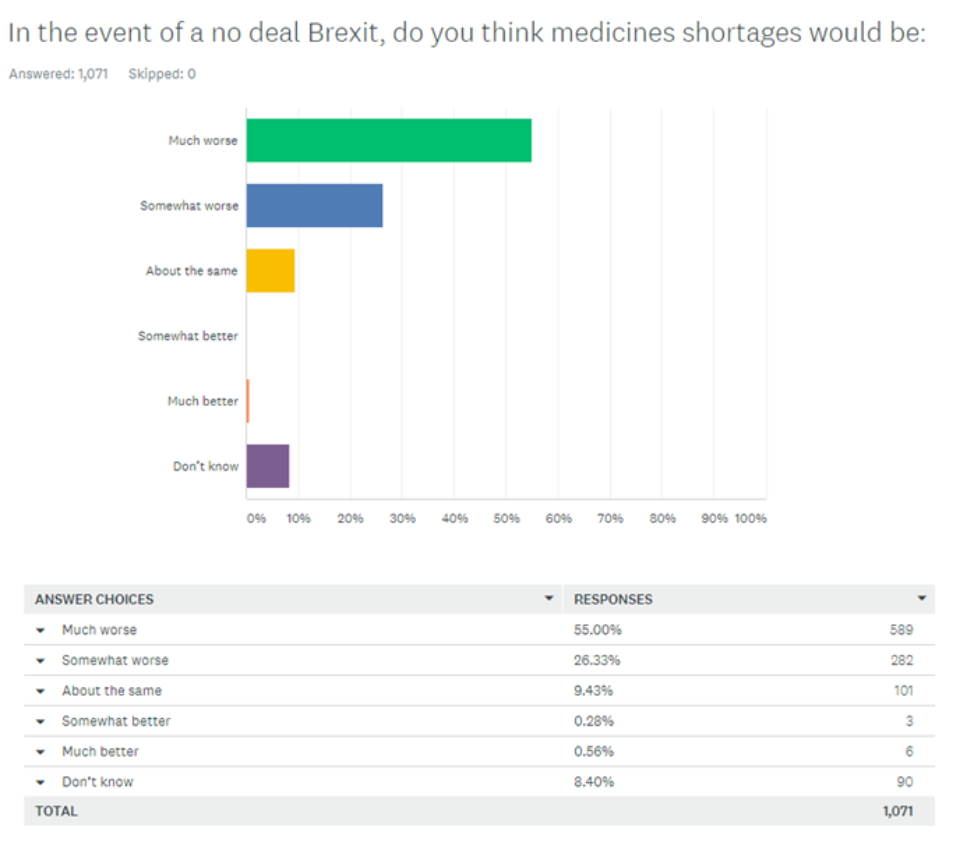
Figure 5: Pharmacists’ expectation of consequences from a no deal Brexit
Comments
Some comments from respondents included:
- The very significant increase in medicine shortages has been noted by patients and I daily am asked if it is because of Brexit. I cannot answer as I have no information on why it is happening. But it is taking up ever more of my time – trying to source, getting Rx for alternatives & having increasing numbers of confrontational patients taking their anger & blame out on me & my staff. This further reduces morale in a sector where it is already low.
- I work as an antimicrobial pharmacist in secondary care and dealing with medication shortages are part of my daily tasks now. The situation is becoming critical and I believe has serious consequences to patients. I’m not sure if Brexit has resulted in some issues at present but worry it may worsen.
- As well as taking 2 hrs of my time shortages almost take a whole dispensers time every day
- (from a hospital pharmacist) I have a lot of national contracts being withdrawn or changes for hospital supply, often with no notice given. Have increased buying staff from 2 people to 5 people within the last 3 months to cope with the demands of the procurement office to keep pace with work.
- I think the SSPs [Serious Shortage Protocols] will be for only a minority of items and will not be time to deal with problems. A lot will need to be done at a local level at short notice in response to local shortages. Not sure what the government has really done to prepare and I think problems will not be resolved after the 6-week stockpile is exhausted and the cross channel is not supposed to sort for 6 months.
- Can’t wait to retire. After 40 years in the job, I have never before felt so down. I now get shouted at daily by customers. Not pleasant.
- Community pharmacists are seriously struggling to provide a basic dispensing service. This is the service that most of our patients most want most of the time.
- Community pharmacists are struggling with their workloads already.
- Definite increase in medicine shortages including significant drugs such as adrenaline.
- The amount of repeated workload is unfathomable, we spend hours a day chasing out of stocks in one single 900 item chemist. 1 item can turn into 10 times the work to repeatedly chase 3 suppliers we use + inform the patient + check in again week after week. Furthermore, we refer patients back to GP’s to find an alternative but the GP has no idea what’s in stock. GP surgeries and hospital doctors should have access to livestock figures to prevent the situation at step 1.
- Wholesalers and manufacturers should post bulletins of suspected future stock shortages to the prescribers themselves so they can plan ahead. The message goes from the wholesale management to the pharmacies alerts and messages, store manager passes them to the pharmacist, pharmacist passes this to the dispensers, dispenser passes this on to the patient, patient passes this on to the receptionist, receptionist passes on to the GP by which time the message is so diluted it no longer makes sense.
- We have had several patients appalled by the lack of plans to deal with medicines shortages and the lack of pressure put on suppliers by big corporate pharmacy chains.
- The situation is becoming critical and I believe has serious consequences to patients. I’m not sure if Brexit has resulted in some issues at present but worry it may worsen.
- The stress being generated by these shortages for both patients and staff is immeasurable. It is adding to the burden of trying to help people.
- I have no confidence that Serious Shortage Protocols would be helpful in managing potential Brexit shortages. Currently, all requests for replacement medication is referred back to the GP surgery for action and they are seldom accompanied by suggestions for suitable alternatives. Where community pharmacists do make alternative recommendations, they are often unsuitable.
- As a large NHS Trust medicines shortages is a huge and increasing problem. We are now employing staff just for this purpose, as MI can no longer keep up. The ability to substitute for another medicine is good but it assumes that the other is available and may impact on patients on this treatment. Escalation costs is another huge concern, as pressure and demand on the system increases who will manage costs? It is also impacting on research, how do we continue to recruit patients to trials on specific molecules but be at risk as these cannot be changed and therefore reduces the attractiveness of UK as a research centre.
- I am dreading Brexit because patients already blame us for the shortages, they don’t realise feckless politicians are lying to them and are responsible for the problems.
- A lot of shortages are the result of wholesalers keeping insufficient stock. They rely on a just in time delivery with little or no backup. This needs to change so there less supplier delivery failure even when the manufacturer has sufficient stock.
- There should be a site to show what drugs are available and what aren’t. CCGs implement drug switches and a national roll-out could be carried out to automatically switch to available drugs rather than making patients, pharmacists and GP scratch heads on alternative routes whereas that time wasted can be used to treat/do something constructive than just chase stock. It’s quite naive of industries/drug manufacturers not to have stock. I believe they have statistics to show what quantities are being dispensed in the market hence control production.
- Hospital pharmacy is deeply underprepared in my humble opinion. The carter report led to reduced stockpiling which is good for reducing shortages overall but, combined with chronic understaffing, means district generals are far more vulnerable to intermittent shortages.
- As a locum, I have had big problems with supplies due to quotas and ‘no right to buy’ by wholesalers and manufacturers. Surely this is restrictive practice ?
Notes
Note: A total of 1,071 pharmacists responded to the survey (from 22 August – 27 September 2019)
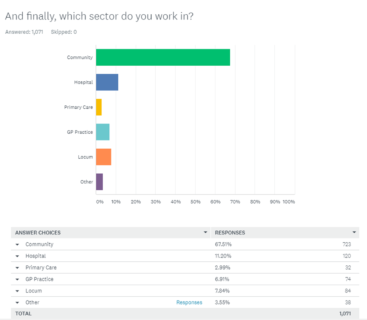
Figure 6: Part of sector where respondents work